






Laparoscopic Nissen Fundoplication
Nissen Fundoplication surgery is a procedure to treat gastroesophageal reflux disease (GERD). GERD occurs when stomach contents reflux and enter the lower end of the esophagus (LES) due to a relaxed or weakened sphincter. GERD is treatable disease and serious complications may occur if left untreated.
GERD is treatable disease and serious complications may occur if left untreated. GERD is a chronic condition where the stomach contents reflux into the esophagus. Normally, the stomach contents do not enter the esophagus (food pipe) due to a constricted lower esophageal sphincter. In GERD, the LES is weak or relaxed enabling stomach acids to reflux into the esophagus.
The main symptom of GERD is heartburn. Heartburn is a form of indigestion. It is usually felt as a burning pain in the center of the chest. Other symptoms can include:
- An acid, sour taste in the mouth
- Burning pain in the throat
- Difficulty in eating
- Bloating and belching
- Stomach pains
- Regurgitating food (when food comes out of your stomach and back up your esophagus)
- Nausea and vomiting
- Vomiting blood
- Dark tarry stools
Symptoms tend to get worse after eating, especially after a large fatty meal.
Diagnoses
Your doctor usually diagnoses based on your medical history alone, but may ask you to undertake the following tests:
- Endoscopy- A thin endoscope with a camera on the end is passed down the esophagus towards the stomach. It enables doctors to see the inside of your esophagus on a television monitor.
- Barium x-rays: These are diagnostic x-rays in which barium is used to diagnose abnormalities of the digestive tract. The patient drinks a liquid that contains barium, which will coat the walls of the esophagus and stomach. X-rays are then taken, which can then show if there are strictures, ulcers, hiatal hernias, erosions, or other abnormalities.
- Esophageal manometry: This is a test that measures the function of the lower esophageal sphincter and the motor function of the esophagus.
- PH Study or Acidity test: This is done on the inside of the esophagus by passing a thin wire through your mouth or nose and into your esophagus. The wire will measure how acidic your esophagus is and record the results electronically.
- Ambulatory 24 hr PH Probe Study: This study measures the acid that refluxes back up from the stomach. A very thin tube is inserted up through the nostril and then down the throat and esophagus until it reaches just above the stomach. The tube has a very small probe at the end that will register any acids that are refluxed from the stomach. An x-ray is taken to make sure that the probe has been positioned correctly. The other end of the thin tube is attached to a small computer (small black box) for 12 or 24 hours. During this period, you are given a diary sheet to complete, on which you should record the time of each activity that takes place, basically a running history.
- PH Capsule: This is a new type of pH probe which requires no tube though the nose. It is a sensor that is attached to the lining of the esophagus, with an endoscope. Often this procedure is carried out at the same time as having an endoscopy (upper GI) performed. The pH sensor sends signals to a portable computer which collects the data about the acid exposure over the usual 24 hrs. There is no removal procedure, the sensor will slowly detach itself from the esophagus with time and is then passed through a normal stool.
- Impedance Study: Similar to a standard pH test, but with two probes. One sits in the stomach and the other just above the stomach. The advantage of the dual sensor is that it can detect both acid and alkaline reflux travels. The tube is inserted through the nostril (this can be placed whilst still sedated after an endoscopy), and the other end is attached to a small computer, no bigger than a Walkman.
Surgical Introduction
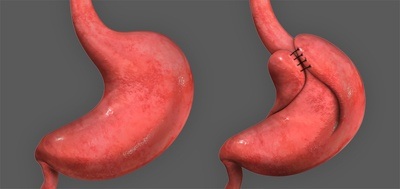
If conservative treatment options fail to resolve your GERD, your doctor may recommend a surgical procedure called Nissen Fundoplication. Nissen Fundoplication surgery reinforces the lower esophageal sphincter’s ability to close and helps to prevent gastroesophageal reflux from occurring. The surgery involves wrapping the top part of the stomach, the fundus, around the lower end of the esophagus and suturing it in place. Sutures are also placed to narrow the hiatus, the opening in the diaphragm that the esophagus passes through, to prevent or treat concurrent hiatal hernia. Hiatal hernia is a condition that occurs when the upper part of the stomach slides up into the esophagus.
This surgery can be performed laparoscopically through tiny incisions in the abdomen as opposed to an “open” approach with a large abdominal incision. A laparoscope is a long, narrow telescope with a light source and video camera at the end. The scope is passed through a tiny incision into the abdomen where images from the camera are projected onto a large monitor for the surgeon to view. Laparoscopes have channels inside the scope enabling the surgeon to pass gas in and out to expand the viewing area or to insert tiny surgical instruments for treatment purposes. The surgical instruments used in operative laparoscopy are very small but appear much larger when viewed through a laparoscope.
Surgical Procedure
Nissen Fundoplication is performed as day surgery either in the hospital or outpatient surgery center usually with the patient under general anesthesia.
- The surgeon uses a needle to inject a harmless gas into the abdominal cavity near the belly button to expand the viewing area of the abdomen giving the surgeon a clear view and room to work.
- The surgeon makes a small incision in the upper abdomen and inserts a tube called a trocar through which the laparoscope is introduced into the abdomen.
- Additional small incisions may be made for a variety of surgical instruments to be used during the procedure.
- With the images from the laparoscope as a guide, your surgeon wraps the upper part of the stomach, the fundus, around the lower esophagus to create a valve, suturing it in place.
- The hole in the diaphragm through which the esophagus passes is then tightened with sutures.
- The laparoscope and other instruments are removed and the gas released.
- The tiny incisions are closed and covered with small bandages.
Laparoscopy is much less traumatic to the muscles and soft tissues than the traditional method of surgically opening the abdomen with long incisions (open techniques).